Plantar Fasciitis / Heel Pain/ Heel SpursMany people can suffer from Plantar Fasciitis at some point in their lives. It is a very common condition that presents itself as pain in front or side of the heel bone (Calcaneus).What is Plantar Fascia?The soles of our feet have a tough complex layer of Plantar Fascia (PF). This dense fascial web creates a flexible springy cushion under the soles of our feet. It protects the bones by reducing impact and reinforcing the musculature giving our feet strength and resilience. It connects the bones of our toes to the Calcaneus, merging into the Achilles tendon and calf. In Anatomy Trains this is just one part of the Superficial Back Line. (Image showing part of Superficial Back Line in Anatomy Trains, Myers 2000)What is Plantar Fasciitis / Plantar Heel Pain / Heel Spurs?Plantar Fasciitis is the medical term for thickening of the Plantar Fascia (PF) in the sole of the foot. The thickening causes shortness in the length and breadth of sole pulling the Calcaneus forward causing inflammation - Plantar Heel Pain. If untreated Heal Spurs can also develop. The thickened / shortened PF pulls the heel bone forward towards the toes, it tugs on the periosteum (membrane) of the Calcaneus creating a gap between the edge of the Calcaneus and periosteum. Over time Osteoblasts fill this gap with new bone which forms into a Heel Spur. (Image from Anatomy Trains, Myers 2000)The cause of pain underneath the foot and heel is commonly suggested to be from over-use, weight gain and age. KMI Structural Integration Practitioners can recognise the signs and treat before the pain begins, meaning Plantar Fasciitis, Heel Pain and Heel Spurs are unlikely to develop. In practice it is extremely common to find feet that are stiff and tight. Their movement into dorsi flexion (lifting foot/toes towards head) and plantar flexion (pointing toes/foot towards floor) is limited and the arches of the foot have lost their spring. If left untreated and an individual either over-uses their feet and/or increases in body weight, the PF may begin to show signs of strain resulting in Plantar Fasciitis.When we walk, run and play; feet are our shock absorbers, they need to be flexible. The arches should be sprung to allow the foot to spread on impact and propel us forward on strike off. Over time the whole foot can lose its shock absorbing ability. This could be due the types of shoes worn which prevent the foot from moving freely; physical inactivity; poor flexibility and tightness in the whole Superficial Back Line.Postural Problems Associated with Plantar Fasciitis.Sufferers of Plantar Fasciitis can present aches and pains elsewhere in the body because of subtle subconscious compensations needed to avoid exacerbating the pain. If for example pain is felt in the right heel we naturally avoid putting weight onto this area. Weight may be taken 1; on the sole of the foot, 2; to the inside or outside of the heel or 3; carried through your left foot.Putting weight on the sole of the foot to keep our heels off the ground shortens the calf which is myofascially linked to the sole of the foot through the Achilles tendon. A shortened calf puts more strain on the Achilles tendon, Calcaneus and PF. Although this relieves the pain it shortens the Superficial Back Line further and can make the overall problem worse. Putting more weight onto the inside or outside of the heel avoiding the sore spot directly effects left to right foot balance. Your inside arch will be higher when protecting the inside of the heel, or collapsed if protecting the outside of the heel. The balance of the arch immediately affects the balance of the knee. If the inside arch collapses the knee will also collapse which may develop into a weakness and over time cause uneven wear to the knee joint.Carrying more weight on the left foot, we alter the forces going through the pelvis which impacts spinal function. Optimum pelvis function comes from both horizontal and front-to-back balance. By taking more weight through the left leg, we upset this balance. If this is for a long period of time, we will develop a permanent postural compensation. Pelvis horizontal balance is lost, putting strain on the lumbar vertebrae in the back causing back ache. The left shoulder will become sore causing strain on the right hand side of the neck.These may sound extreme but if the compensations are left un-noticed or worse, untreated problems surface in the knee, lower back, shoulder and neck long after the Plantar Fasciitis has been cured. How can Plantar Fasciitis be cured?Whatever the reason for loss of flexibility in the foot, the wonderful news is that living connective tissue and fascia can be improved. Fascia is a living organism and whilst we are still alive it continually adapts to its environment. Common remedies like stretching the sole of the foot by rolling it over a ball, lowering the heel off the stairs, hamstring and calf stretches will all help cure Plantar Fasciitis. Taping may also offer some relief by preventing the foot moving beyond its place of comfort straining the inflamed PF.Feet that present these symptoms often feel hard and grainy (like sand paper) beneath the skin to a trained practitioner. This is due to dehydration in the plantar fascia. The beauty of having hands-on KMI Structural Integration is that it can help cure Plantar Fasciitis faster by getting to the root of the problem - thickened and shortened Plantar Fascia (PF). A KMI practitioner will work to specifically increase the length and flexibility of the PF and calf whilst balancing the arches of the foot. The PF will rehydrate regain its suppleness and health. Your whole foot will feel more supple, toes will become more spread apart, you will feel more connected to the ground, your feet will be more comfortable in shoes (or barefoot) and your body will feel like is has a solid base on which to perform all that you ask of it.To find out more, have a free consultation or to experience KMI Structural Integration, please do contact Angela Donovan of Structural Balance via telephone 07950 028 016 or email info@structuralbalance.co.uk.
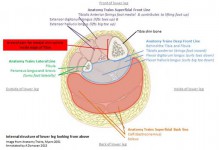
Read MoreDo you suffer from shin splints?It is common for athletes to suffer from shin splints. Many do not know they can be resolved through KMI Structural Integration.Shin splints is a term used to describe medial tibial stress syndrome which is felt as pain and inflammation on the inside or more rarely, outside of the shin bone (tibia). For the lower leg to function correctly all the muscles need to freely slide over each other, expanding and contracting as the foot moves. When tightness or imbalance of these muscles occurs, fascial connections to the tibia become strained causing pain. What is fascia? Please click here for more information.The diagram below shows the anatomy of the lower leg, looking internally from above, below the knee. The area of shin splints being identified by the red box on the left. The lower leg can be split into four fascial compartments published by Tom Myers in Anatomy Trains 2001. Within each fascial compartment, each muscle has its own fascial wrapping. When running, the demand for function is greater, impact and planes of motion increase because of varying terrain and techniques. Incorrect function, over training and/or lack of stretching can lead to muscle tightness. When muscles don’t contract or expand as they should, the fascial wrappings which connect to the periosteum of the tibia become over stretched and strained causing inflammation and pain - shin splints.To relieve shin splints, many sufferers rest and begin running gradually with the aim of improving muscle contractile ability and function. However this may take time and does not work for everyone. KMI Structural Integration can remove these fascial restrictions, release tightness held in the muscles of the lower leg and regain correct function.How is KMI Structural Integration different to a normal massage?Massage is excellent for restoring muscle function and improving blood flow. KMI Structural Integration works at a deeper fascial level. When looking at person with shin splints, the whole gait of the foot and leg is assessed. The aim is not only to relieve the pain of shin splints but also restore correct balance and function of the foot and leg which affects whole body balance and function. To find out more, please contact Angela Donovan of Structural Balance
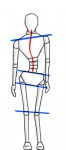
Read MoreIf you are suffering from knee pain, you are not alone - it is a very common complaint. A postural example to share that I often see in practice is where patients have an X leg pattern (below images) ‘knocked knees’. This can be in one or both knees, the example below is showing the right knee. When this happens the pattern seen in the soft tissue is as follows:The L image below shows the right side of the pelvis being lower than the left which we call a right tilt of the pelvis. The alignment of the right knee is being compromised, creating a strain on the inside of the knee. The left hip is higher changing the weight distribution into both legs. Instead of the weight being even through the centre of both legs, the right leg becomes a stabiliser with the line of force moving to the outer edge. The weight distribution into the left leg will be less and the line of force will be to the inside of the leg. Often clients are aware of feeling out of balance when they walk and be experiencing lower back pain. So whats happening in the soft tissue when this happens?The left femur (thigh bone) is held deeply into the hip socket by tight Gluteus Medius and the anterior Adductor muscles. The inner arch of the foot can also lift. In the Anatomy Trains lines, we are looking at tightness in the Deep Front Line below the pelvis. On the right side the deeper muscles underneath the Glutes tighten, Gamelli's and Quadratus Femoris, plus the lateral hamstring - Short Head of the Bicep Femoris (SHBF) and Vastus Lateralis tighten. Over time a fascial adhesion builds between the femur and the SHBF which pulls the knee inward and we experience pain on the inside of the knee and/or underneath the Patellar. Beneath the knee the foot balance is altered dropping the inner arch because the Peroneal’s tighten on the outside of the Fibula reducing ankle mobility and unbalance the calf and Soleus. This is the Anatomy Trains Lateral Line. When this happens we have no option other than to move out of alignment putting our right knee, ankle, hips and spine under strain. Often we are told to strengthen our quads to support our knee but if this imbalance is not corrected, no amount of quad strength will help. Above the pelvis the compensation pattern continues. The left side/waist becomes very tight superficially beacause Quadratus Lumborum and the diaphragm become restricted. The right side of the ribcage becomes restricted and the right Psoas and spinal muscles tighten to stabilise you. This pelvis imbalance is often the primary cause of lower back L4 & L5 spinal problems. The shoulders and neck become compromised too because superficial tightness of the ribcage restricts shoulder movement which tightens our Trapezius and Pectoral muscles and a tight Psoas pulls the neck forward and down creating problems in the C7 Vertebrae area. Standing tall and upright becomes increasingly more difficult. What can help correct knocked knees reducing knee pain?Orthotics can help lift the inner arch of the foot but if used for long period of time also weaken the foot structure. Stretching can help release tight areas and strengthening exercises will assist; but many people do not experience lasting change until the pattern is addressed.KMI Structural Integration can alleviate knee pain and its compensations felt throughout the body. In this example lengthening the stabilising R Lateral Line and releasing the Left Deep Front Line through hands on techniques and movement will bring the pelvis back into horizontal balance and balancing the weight distribution taking strain away from the affected joints.What makes KMI different is the approach of fascial release whilst focusing on whole body alignment which creates lasting change. To find out more, have a free consultation or to experience KMI Structural Integration, please do contact Angela Donovan of Structural Balance via telephone 07950 028 016 or email info@structuralbalance.co.uk.
Read MoreIntroductionBiotensegrity is emerging as the most significant development in human anatomy in recent years.With important ramifications for a wide range of medical practitioners including surgeons, bio-engineers and human movement specialists. Bespoke dissection techniques are providing a new vision and understanding of the continuity of the human form. A fresh look at the human fasciae highlights its role in providing continuous tension throughout its network. The term “Tensegrity” was coined by Buckminster Fuller combining the words ‘tension’ and ‘integrity’. Fuller’s student Kenneth Snelson built the first floating compression structure of “tensegrity” in 1949 while Dr Stephen Levin an orthopedic surgeon was the protagonist of “BioTensegrity” in the early 1970’s. As a Clinical Anatomist I have investigated this model and the role of fascia in my dissections to better understand the mechanisms of human movement and chronic pain while providing new anatomical knowledge and awareness leading to less invasive surgical and non-surgical therapeutic interventions.Please refer to attached pdf for remainder of article... BioTensegrity Fallacy of Biomechanics.Sharkey.pdfCorrespondence to: John Sharkey MSc. University of Chester/National Training Centre 16a St Joseph’s Parade, Dorset St, Dublin 7, Ireland. E-mail address: john.sharkey@ntc.ie. Website: www.johnsharkeyevents.com
Read MoreIntroductionProfessional bodyworkers, exercise and movement practitioners follow a standard protocol for the treatment of acute injury. RICE. Rest, Ice, Compression and Elevation. Since its widespread introduction in the seventies we have witnessed a plethora of variations on this theme including PRICE (P for prevention) and RICER (R for referral) and others. Readers would be forgiven for thinking there must be a plethora of gold standard, peer reviewed research supporting the use of ICE on newly aquired, swollen tissues.The anagram RICE comes from one source, a book written in 1978 with the title Sports Medicine Book penned by Dr Gabe Mirkin (an excellent book, by the way). In the tradition of good science practice Dr. Mirkin has raised a hand to say he may have got it wrong. Now Dr. Mirkin has a web-site (www.drmirkin.com/ fitness/why-ice-delays-recovery.html) devoted to letting people know that the anagram RICE, catchy and all as it is, was just an idea, his idea. Of course he thought it was a good idea at that time and he was correct, it was a brilliant idea. In spite of the fact that there was no research supporting the idea, just a catchy anagram, it has prevailed to the present day as if it were the only word or the last word concerning standard protocol for treating acute injury.This raises the question: ‘What other paradigms are we using that have no basis in fact or are not supported by empirical science’? Is it time to expand our understanding and explanations of human anatomy, physiology and motion guided by the new evidence coming from sources such as Biotensegrity-anatomy for the 21st century? Have we heard the only word or the last word when it comes to accepted paradigms or has the time come to update our positions and our thinking based upon our newly-found understanding of human anatomy and physiology?Please refer to attached pdf for remainder of article.. John Sharkey M&MA Journal Summer 2017-2.pdfCorrespondence to: John Sharkey MSc. University of Chester/National Training Centre 16a St Joseph’s Parade, Dorset St, Dublin 7, Ireland. E-mail address: john.sharkey@ntc.ie. Website: www.johnsharkeyevents.com
Read More“Discovery consists of seeing what everybody has seen, and thinking what nobody has thought’’ (Albert Szent-Gyorgyi). This is true of Dr. Stephen M.Levin M.D an orthopedic and spine surgeon. Dr. Levin former ClinicalAssociate Professor at Michigan State University and Howard University, originated the concept of Biotensegrity 40 years ago"IntroductionIn the first article of this three-part series I provided a basic explanation of BioTensegrity. While a growing number of professionals are beginning to understand what Tensegrity is, a wider population of bodywork and movement therapists need to know what it is not. Bodywork and movement therapists also want to understand how they can integrate BioTensegrity into their specific model of movement and bodywork within their clinical practice. Understanding BioTensegrity has wide reaching implications for massage therapists of all stripes and for medical specialists including surgeons. The father of biomechanics was born 28 January 1608 and following his death in 1679(penniless and destitute), Giovanni Alfonso Borelli left behind a legacy that would prevail to the present day. BioTensegrity claims more than a tincture of skepticism when it comes to the classic descriptions of animal movement and human biomechanics as promoted by Borelli.Please refer to attached pdf for remainder of article... John Sharkey Myotherapy Aust 2015.pdfCorrespondence to: John Sharkey MSc. University of Chester/National Training Centre 16a St Joseph’s Parade, Dorset St, Dublin 7, Ireland. E-mail address: john.sharkey@ntc.ie. Website: www.johnsharkeyevents.com
Read More