Here goes. I’m jumping into the shark tank! So, a bit ago I was privy to an email that was sent by a student of Structural Integration (let’s name them “Nat” to protect the innocent) to one of my SI students. I don’t know completely the reason Nat reached out my student; it might have been to get a sense of our SI training and ‘size us up’ so to speak.In the email, Nat mentioned how they were studying to be a Rolfer™ in the San Francisco Bay Area. I was instantly intrigued as there is no Rolfing training here (as of May 2018). What struck me more was the rest of the email text. Nat proceeded to mention how they were studying from a practitioner who did not attend the Rolf Institute and is not a Rolfing instructor. But Nat considered themselves to be studying the “pure Ida Rolf ‘recipe’ that is taught at the Guild.” This, unfortunately, is not the first time I’ve heard this sentiment from people who have not studied at The Rolf Institute. Before I go further, I want to be clear about which “shark tank” I’m actually jumping into. This is not about Rolfing® vs. the Guild or Rolfers vs. everyone else. This is about respect for a trademark vs. non-respect for a trademark which is often disguised as traditionalism. My first thought reading the email was, “Wow. So many lessons to be learned.” It’s important to understand a tiny bit of history before I go further. Early in the history of Structural Integration, two main teachers (Emmet Hutchins and Peter Melchior) broke off from the Rolf Institute to form their own school, the Guild for Structural Integration. They have both passed away and I never met them. I did meet Peter Melchior’s daughter once. As I’ve been told, they were amazing teachers and I’m sure we have lost two true masters of the craft. Since then, other people who have taught (or have been students) at the Rolf Institute have gone on to form their own schools.I won’t go into the whole entire timeline because frankly I don’t know it completely, but I will suggest the book “Rolfing and Physical Reality” by Ida Rolf if you want to get a sense of her early history.In fact, the purpose of this article is to state that the whole entire history of how the “cell divided” is not as important as people may think. I’ll repeat this in different terms and address it to the Nats of the world: It doesn’t matter what you believe as far as who’s the “real Rolfer” or who was gifted to carry on the “pure recipe.” And here’s why: At some point in history The Rolf Institute trademarked the terms Rolfing® and Certified Rolfer™. The Rolf Institute then became the only organization who could use the terms or grant license to the use of those terms.At that precise moment the entire debate of who is a “real Rolfer” or what was “pure” ceased to be defined solely by the lineage of the craft (I’m the real Rolfer because I studied under so and so….NO I’M THE REAL ROLFER!). This is because U.S. Trademark Law now comes into play. I sure hope Nat is reading this and they understand. The fact that The Rolf Institute has been granted a trademark leaves the debate of who is “real” and who is not “real” back in the past. At this point, it’s probably important for me to describe my lineage and my path. I studied at the Rolf Institute in 2007-2008 in Boulder, Colorado, and Brazil, under amazing teachers like Jan Sultan, Monica Caspari, and Kevin McCoy. I went back to the Rolf Institute in 2015 to train as a Certified Advanced Rolfer™ with two masters, Russell Stolzoff and Ray McCall. I wouldn’t trade those experiences for anything else. As I mentioned, the term Certified Rolfer™ is a trademark and requires an annual license fee to be paid which I gladly pay every year.Afterwards, I created my own school of Structural Integration, the Morales Method® Academy of Structural Integration. My school and my teachings are a branch directly from the teachings at The Rolf Institute. I went off in my own direction and teach Structural Integration from a different approach. I share my lineage and history in my program, called MMASI.It would be silly and immature to call what we do at MMASI “real Rolfing” or even to extract the “pure recipe” from another training (yes, I do know it) and trumpet what I teach as the “pure recipe.” In fact, I like to describe the differences between what I teach and what I was taught because I feel it’s important for everyone to understand the distinctions. In our philosophy, evolution is welcomed and we feel it makes progress possible. Enough of MMASI though, let’s go back to the main reason for this article.Rather than attempt to reach one person (and possibly a person who has already swallowed their dogma—hook, line, and sinker), I am writing this to reach a larger audience. May I give those who believe one method of SI is “purer” or “better” than another a bit of advice: Focus on studying the craft of Structural Integration instead of trying to measure your studies (and quite possibly yourself) against Rolfing or other forms of SI.What’s the obsession over Rolfing anyway? Be happy in your studies. I’m sure you’re learning great stuff, but don’t call what you’re doing Rolfing unless you’ve graduated from The Rolf Institute. It’s not a good look.One more thing. Nat mentioned in the email that these “real Rolfers” (who are training Nat) have received Cease and Desist letters from the Rolf Institute which they “immediately make into paper airplanes and score 3-point garbage can shots.” Apparently, this group does not adhere to, or respect, U.S. Trademark Law.Wow. So many lessons to be learned.
Read MoreNext ISM Class Begins in 2019We offer a four-year, 2,108-hour practitioner training program, culminating in certification as a Structural Medicine Specialist.TM The program consists of eight to nine five-day weekends per year, held in Twisp, Washington. After the second and third year, there is a retreat intensive. Some training may take place in the Seattle area. Between segments and practicum, students engage in Independent Study and document their findings in short essays. Learn about our training program, career rewards and application process.
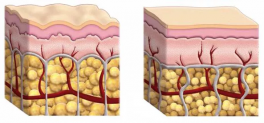
Read MoreIf I had a nickel every time someone asked me about cellulite I would probably be able to take my wife out for ice cream (in San Francisco!).I’ve talked with a lot of clients and students about this topic and I thought I’d throw my hat in the ring so to speak and let you know what comes to the mind of a bodyworker who has studied fascia up close and personal (ie dissection) with regards to cellulite.First off, let’s agree that cellulite is a ‘dimpling’ of the skin. Where it resides on the human body and the percentage of men vs women who get cellulite is out there so I won’t into the stats. Those who have it know full well where it’s hanging out!Let’s go back to this dimpling part. And let’s do this by looking at this image above. The image on the left shows the dimpling we know so well. The image on the right shows smooth skin. What’s the big difference between the two? There are a couple of major things to note here. First off, the yellow circles are bigger on the left hand side image compared to the right. Those yellow circles represent fat cells. The other major difference are those white vertical lines. Those lines represent collagen fibers, often called Connective Tissue (or, Fascia). When adipose tissue (fat, again, as seen by those yellowish spheres) becomes larger, they crowd up to the surface layer of the skin, making the collagen fibers taut. Some fibers will give more than other fibers and you will see a ‘dimpling’ in the skin. Imagine a seat cushion like this one:In this seat cushion you can imagine that the areas where the cushion is pinched inwards is doing so because the there is a string/thread that doesn’t let the cushion plump. That’s what the collagen fibers/connective tissue could be like inside a person. The dimpling in the cushion can represent the dimpling of cellulite. Some fibers may be longer or have more room to give than others and thus some areas bulge out more than others. Couple that with oversize fat cells and you’ve got some dimpling! So let’s move on.In the case of the seat cushion I could just snip the threads that pinched inwards and the seat cushion wouldn’t have the same look as before. In the case of the human body those threads are the vertical white lines that are made up of collagen fibers.Collagen is extremely strong. So strong in fact that it has the tensile strength (the resistance to break under tension) of soft steel (pound for pound about 42,000 lbs per square inch). That’s incredibly strong.And here’s what we know so far about cellulite. In order to get rid of the condition there are two things that can be done:1. Decrease the size of the fat cells (this can be done by decreasing the deposit of fat through diet and exercise).2. Cut the collagen fibers that are contributing to the dimpling effect.That’s pretty much it folks. Let’s breakdown option number 1.With option number 1 the person would have to change the way they eat (less calories) and increase their physical activity. Dieting has been documented to have mixed efficacy. Just remember back to the last time you dieted and you’ll know how difficult it is to maintain a certain weight after dieting.With option number 2 we need to go back to the fact that collagen fibers are extremely strong. In order to cut or snip those fibers we would need a cutting tool. Right now an effective cutting tool for this type of issue is a laser cutting tool so it makes sense that most effective methods for cellulite treatment involve laser cutting. The laser penetrates under the skin layer and trims collagen fibers. The adipose cells then are free to plump in the areas where they were previously restricted and the look of cellulite is diminished. Some laser machines also involve suction and skin manipulation. The medical/cosmetic community is still gathering data on this process as more patients undergo the treatment.So, now that we know what can work with cellulite what about all those other options we see on late night tv? All other options fall under two categories, manual therapy alone and plastic tools, both meant to treat cellulite. The effectiveness of both can be addressed together.Because of what we know about the strength of the collagen fibers (yes, it’s a fact) no amount of pressure from an elbow via manual therapy or any plastic tool (no matter how vigorously your scrape away at yourself) will ever tear at the collagen fibers. Maybe something like this could do it though:So, you might be thinking: “Marty if you’re so right then how come when I use my (insert latest name of fascial therapy plastic for sale out there) that it looks like my cellulite is gone?!”Well, I’ve got an idea as to what’s happening. If someone vigorously scrapes their skin and does so with enough depth and enough force, they will create an inflammation effect. The skin will become red, swollen, and inflamed. In this case, the look of cellulite will diminish because the swelling has plumped up the tissue. After being sued for deceptive advertising, one maker of these scrapers changed their tune and stated that their product “diminishes the appearance of cellulite” after originally claiming to getting rid of cellulite. So what’s a person to do if they have cellulite? Well, proper diet and exercise could help but it’s not a guarantee. The other choice is to live your life knowing I (and I’m sure countless other people) care for you and think you’re a pretty cool person regardless of how taut your collagen fibers are. <3
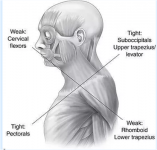
Read MoreJanuary 19, 2018 written by Marty MoralesDr. Vladimir Janda’s Upper Crossed Syndrome was an eye opener for many practitioners. In it Dr. Janda stated that a syndrome occurred when people were exhibiting slumped shoulders. Not only were the shoulders slumped but a muscle imbalance and muscle weakness pattern arose. This combination lead the way to Dr. Janda creating an approach to slumped shoulders that included assessment of the shoulder regain along with exercises to strengthen weak muscles. Practitioners of manual therapy have stepped in as well, using their skills and modalities to address soft tissue tightness. But is this where the story ends? For the Structural Integration (SI) practitioner, this is the beginning of the story.In this article we will explore the potential for further work using the Upper Crossed Syndrome as a model and exploring two different ways of working from an SI point of view.Upper Crossed and Directional ResistanceSo, let’s say we’ve got a client with Upper Crossed Syndrome (UCS). They may typically exhibit the posture as seen in the image above. As Dr. Janda pointed out there’s tightness in the pectoralis area and in the upper trapezius area. In the MMASI form of SI, we deal with a term called, Directional Resistance. Directional Resistance is the palpatory sensation you get when you sink into tissue (into end range) and you feel that the tissue resistance in one specific direction. The idea of Directional Resistance permeates through the whole of the Morales Method of SI and allows the SI practitioner to work from a ‘functional’ perspective. Why is this important? Let me describe a common scenario (not 100% of the time but this is a common scenario) that happens with UCS. I may usually see a client with the typical UCS and they may look a bit like this:Source: As I start to palpate the pectoralis tissue and the upper trapezius tissue, keeping Directional Resistance (DR) in mind, I find that the DR will go in this pattern:Meaning the tissue will be resistant in the superior direction in the anterior territory and will be resistant in the inferior direction in the posterior territory. I may then start to work in the direction of resistance, going superior (or superior-lateral if the case may be) and inferior (or inferior-lateral if the case may be) in order to create movement or fluidity in the direction of resistance. The objective here is to create the option or possibility for the shoulder to not have to round. Work including the arm in order to involve the scapula is also included in this work. When an appendage (like the humerus in this case) is utilized, care is taken to understand how the rotation of humerus may affect the palpation of the DR of the tissue being worked.How Do We Know Where To Work?The Janda approach is great at describing areas to work but as we’ve seen, it may not be necessary to work all of the pectoralis tissue and it may not be feasible time-wise to spend effort working every square centimeter of tissue in the anterior and posterior territories.For this reason I teach my students to use the secret weapon of manual therapists: Palpation.Instead of working ALL of the pectoralis, I encourage my students to follow this method: Sink to the tissue and palpate to feel where on the pectoralis you feel the MOST DR. Use that as your starting place. Stay at the level of depth that you feel is END RANGE and work in the DR. Slow and steady wins the race.While working the anterior area, you can keep one hand on the pectoralis tissue while the hand moves the client’s arm. As you’re moving the client’s arm in abduction and/or extension, feel with your other hand where the tissue of the pectoralis doesn’t want to move. This is where you might want to work. Follow steps 1 and 2 above.The same can be done on the posterior territory. You can move the client’s arm as before but also move the scapula.When moving the scapula, have your hand on the rhomboid area to feel for the DR of the upper trapezius, rhomboids, and lower trapezius.You can also have your hand in the territories listed in #5 while moving the client’s humerus UCS and SIBesides using the approach of DR to work UCS, we can also look at UCS from a global perspective, as it is seen when performing SI work. Before we discuss SI strategies, let’s first ask ourselves two questions with regards to UCS.When looking at a client with UCS, would we assume that the rest of their body is in ‘normal’ alignment?If we answered ‘no’ to question #1, then why are we not working UCS involving the whole body?A glimpse into the world of SI: SI practitioners see UCS as not just an upper body issue but as a WHOLE BODY ISSUE. Would we expect this? When SI practitioners look at UCS, we look at how the following main body parts will affect the shoulder girdle:HamstringsTalusPelvic Girdle (this can be shifted forward as a result of the client attempting to find balance in gravityAtlasAbdominal tissue (superficial and deep) and visceral tissueResting eye position (the client may have a different orientation to horizon and may need to adjust it in response to a change in their shoulder girdle These are just a few of the places an SI practitioner may look at when addressing UCS (in addition to the territories the Janda Approach looks at). Keep these in mind when working with your clients. Your client is not just the sum of their parts. They are a dynamic being with many intersections and relationships that make bodywork a rewarding and challenging craft.Original article can be viewed on Marty's blog here
Read More